CASE OF A 42 YEAR OLD FEMALE WITH MULTIPLE HEALTH EVENTS SINCE BIRTH
Case of a 42 year old female with multiple health events since birth
Presented By: Simran Dash
MBBS- IV | Roll number: 153
Present Complaints of the patient :
1) Migraine with aura
2) Swelling which is mainly confined to face and abdomen
3) Sleep disturbances
4) Weakness on exertion
5) Increased tolerance to pain
Description of each complaint in detail :-
1) Migraine with Aura :
- Onset - Sudden
- Duration - Since 2 years of age so approximately 40 years
- Progression - gradually progressive in intensity
- Site - More in the left side
- Associated complaints -
- preceded by Aura,
- generally associated with numbness of left hand and left face
- feeling of rotation and spinning while sleeping on left side.
- Past History : At age of 34 years, she had the worst headache as described by her due to which she lost her vision and began stuttering. It relieved by itself within 2 hours but her stuttering returned.
- She also had mild memory loss as well as loss of function of left side ( dropping things intermittently and severe cramping of left arm.)
- Also had a history of CSF rhinorrhoea from her left nostril.
- At 41 years, she underwent genetic testing and was found to have G6PD deficiency, AMPD1 deficiency, MTHFR deficiency
- Relieving Factors - Triptans
So from the above complaints the possible diagnosis could be :
- HEMIPLEGIC MIGRAINE
- Transient Ischemic Attack (But if she has TIA she is less likely to have other aura symptoms)
- Infections like meningitis, encephalitis (she should have a fever, rash)
- Brain tumours
- Seizures with post-ictal paralysis
- Metabolic Disturbances like Homocystinuria (as she has MTHFR deficiency, she can have high homocysteine levels)
- MELAS ( Mitochondrial Encephalopathy Lactic Acidosis and Stroke like episodes)
In order to confirm the above diagnoses, the possible investigations needed would include:
- CT and MRI of brain can confirm brain tumours, stroke, TIA
- CSF analysis to diagnose infections
- EEG to detect seizures
- Magnetic Resonance Angiography to diagnose TIA
- Intracranial pressure
Possible treatment modalities are :
- Hemiplegic migraine - Triptans (which she is already consuming)
- Surgery (Carotid endareterectomy) - TIA ( cannot give anticoagulants because she has G6PD Deficiency)
- Anti epileptics - Seizures
2) Swelling:
- Onset - since 1 year of age
- Duration - approximately 40 years
- Site - Face , Abdomen
- Aggravating Factors -
- Emotional Stress
- Eating wrong food such as Fava beans
- Exercise
- Smoke
- Relieving Factors - Rest
- Associated factors - Shortness of breath, Decreased urination(increased on fasting), Dark coloured urine on exercise
Possible causes for swelling:
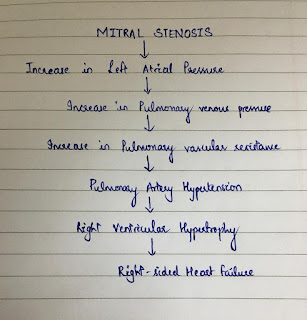
- Since she has hemolytic anemia , she could have Right Heart Failure which is responsible for ascites and shortness of breath (because of Pulmonary artery hypertension).
- And the hemolytic anemia could be responsible for her kidney infection because G6PD is responsible for production of NADPH. And since she has deficiency of G6PD, She does not have enough NADPH and ATP which resulted in loss of lots of ions thereby causing decrease in urination and Facial edema. ( refer to edited paragraph -1 )
- It increased on emotional stress and eating fava beans because she has G6PD Deficiency.
- Her shortness of breath could also be attributed to hiatal hernia.
- Dark urine on exercise is suggestive of hemolysis which could be due to G6PD deficiency.
Differential diagnoses :
- Could be Angioedema
Investigations done in this case are :
- Hemogram - shows anemia
- ECG - signs of Right Heart Failure
- CXR - Left atrial enlargement in this case
- SGPT, SGOT - elevated in this case suggestive of hemolysis
- CUE - to show infection
Further investigations required are :
- LDH -should be elevated To detect hemolysis
- Total BIlirubin - should be elevated
- Reticulocyte count - elevated
- Urobilinogen
- Heinz bodies in RBC on complete blood film
- Beutler fluoroscent spot test - rapid test that identifies NADPH production by G6PD under UV Light
- Haptoglobin ( decreased in hemolysis)
- Direct Coomb's test - negative (suggestive of non autoimmune hemolytic anemia)
- G6PD test
- Skin tests for allergy (for angioedema)
Treatment :
- Avoiding stress
- Do not consume fava beans, sulpha drugs, antimalarials
- Serine- increased urination
- Excess salt consumption
3) Sleep disturbances:
- Onset - since birth
- Duration of sleep - 2-4 hours and no REM sleep
Possible causes :
- AMPD1 Deficiency can cause sleep disturbances because Adenosine is an inhibitory neurotransmitter so it should help in sleep.
- G6PD Deficiency impaired the glycolysis so glycine is not formed well . Glycine is also an inhibitory neurotransmitter.
Treatment taken by her :
- L serine : works like glycine in brain so helps in better sleep
- Cimetidine
4) Exercise Induced Fatigue :
Possible causes :
- AMPD1 deficiency - lack of ATP hence the person gets easily tired.
- Oxidative stress from excess of free radicals because of G6PD deficiency
- Past history shows parents to be chain smokers which increases the oxidative stress.
Treatment given :
- Ribose - helped her too because it provides ATP.
5) Increased tolerance to pain :
- Onset - since 4 years of age ( cannot localize pain even now)
- Associated complaints -
- History of multiple falls
- fracture of ankle
- Never sweats
Differential Diagnosis:
- CIPA (Congenital Intolerance to Pain With Anhydrosis)
- Osteoarthritis could be responsible for multiple fractures. ( refer to edited paragraph -2 )
Investigations required :
- Genetic testing for CIPA (NTRK 1 gene mutation can cause CIPA)
- X Rays of limbs to diagnose osteoarthritis.
Treatment :
- There is no treatment for CIPA so attention should be given to injuries to prevent infection and worsening injuries.
Other problems of the patient:
- PCOS - Responsible for :
- Dysmenorrhoea
- Ectopic Pregnancy
- Increased Hair loss
- Bipolar disorders, Anxiety, Depression - could be because of less sleep and MTHFR mutation (Methylene Tetrahydrfolate Reductase Deficiency)
- Rashes in face (could be SLE)
- ADHD (Attention Deficit Hyperactivity Disease ) - Because of ANKK 1 mutation.
- VWF mutation (Von Willebrand Factor ) - could be responsible for dysmenorrhoea.
The patient should go for whole genome sequencing to find out the other mutations.
EDITS :
1) G6PD deficiency might be responsible for her kidney infection because G6PD is the key regulatory enzyme in the HMP shunt with the production of NADPH that is required for protection against oxidative stress. Increased oxidative stress has been observed in many diseases including those related to renal damage. There is a higher prevalence of the G6PD deficiency in people with unexplained chronic kidney disease. In G6PD deficiency, massive intravascular hemolysis can cause acute renal failure, and acute tubular necrosis might complicate the severe hemolytic anemia.
2) Osteoporosis could be responsible for her multiple fractures. In order to diagnose it, her serum Calcium levels must be checked. And since she has PCOS, she might be consuming OCPs which can decrease the Bone mineral density.
RECENT UPDATES IN THE CASE AS OF MAY,2020 :
Presented with the Complaints of :
1) Oral ulcers
2) Vaginal ulcer
Duration : 1 year
She guessed it was Behçet’s disease last year while discussing with her doctor.
She got diagnosed with Behçet’s disease yesterday on the basis of the following criteria:
Normally the characteristics required to diagnose Behcets include :
1) Mouth sores that have recurred at least 3 times in 12 months is necessary for a diagnosis of Behcets.
2) In addition, at least two of the following symptoms must be present :
i) Recurring Genital sores
ii) Eye inflammations
iii) Skin sores
https://www.mayoclinic.org/diseases-conditions/behcets-disease/diagnosis-treatment/drc-20351331
Since she has complaints of recurring mouth ulcers and vaginal ulcers previously too. She also underwent a pathergy test which confirmed her of having Behcets.
Possible causes for Behcets : She has multiple mutations making her susceptible to various autoimmune diseases like Behcets.
Symptoms which could be associated with Behcets in this patient are :
1) Headache- Because Behcets is characterised by inflammation within the brain (meningoencephalitis) which can cause a very severe headache associated with poor vision, ataxia, difficulty in speaking.
https://behcets.org.uk/information-for-patients/headache-in-behcets-disease/
2) Poor vision - Behcets is associated with Uveitis. That could be responsible for her poor vision.
3) Personality changes - Sometimes it might be the first symptom which should suggest Behçet’s disease.
Differentials for her complaints could be :
1) Herpes Simplex Labialis
2) Aphthous ulcers
3) SLE (also complains of rash on face)
Investigations required for the above diagnoses are:
1) Mainly based on clinical findings such as oral ulcers, genital ulcers.
2) Skin lesions such as acne, folliculitis, malar rash which are suggestive of SL
3) CSF Analysis which might show lymphocytosis In the case of Herpes Simplex Labialis.
4) CT and MRI may show periventricular white matter atrophy and lesions in the basal ganglia.
5) ESR ( elevated because of inflammation)
6) Complete ocular examination to see uveitis
7) Pathergy test (already done by her)
Treatment modalities : It does not have any treatment. The symptoms can be treated by
i) Topical therapy -
a) Creams for the oral and genital ulcers
b) Eye drops for uveitis
ii) Systemic therapy -
a) Immunosuppressants like Infliximab.
b) High dose corticosteroids.
c) Colchicine can be used for genital ulcers but cannot be used here because of her G6PD deficiency.
iii) Cognitive Behavioural Therapy - which she is undergoing.
REFERENCES:
1) https://www.hopkinsvasculitis.org/types-vasculitis/behcets-disease/
2) https://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1
3) https://en.m.wikipedia.org/wiki/Glucose-6-phosphate_dehydrogenase_deficiency
4) https://rarediseases.org/rare-diseases/hemiplegic-migraine/
5) Davidson’s principles and practice of medicine
6) Harrison’s principles of internal medicine
7) https://www.mayoclinic.org/diseases-conditions/transient-ischemic-attack/diagnosis-treatment/drc-20355684
2) https://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html?m=1
3) https://en.m.wikipedia.org/wiki/Glucose-6-phosphate_dehydrogenase_deficiency
4) https://rarediseases.org/rare-diseases/hemiplegic-migraine/
5) Davidson’s principles and practice of medicine
6) Harrison’s principles of internal medicine
7) https://www.mayoclinic.org/diseases-conditions/transient-ischemic-attack/diagnosis-treatment/drc-20355684
This comment has been removed by the author.
ReplyDeleteThanks for sharing your analysis of the online patient record originally posted by our elective Intern Avinash.
ReplyDeleteA few quick queries:
Is this the current order of the patient's perceived priority of her problems?
"And the hemolytic anemia could be responsible for her kidney infection because G6PD is responsible for production of NADPH."
ReplyDeleteCan you elaborate on the above in terms of mechanisms around NADPH deficiency causing kidney infection if that is what you meant and what is the reported incidence of such occurrences?
Is it "Increased tolerance to pain". If so then how is "CIPA (Congenital Intolerance to Pain With Anhydrosis)" a differential diagnosis here?
ReplyDelete"Osteoarthritis could be responsible for multiple fractures."
ReplyDeleteGuess you meant osteoporosis?
Keep it up and if you make any edits to your blog don't delete the precious portions or anything but just make a new para termed edits to this para on date...
ReplyDeletehttps://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html
ReplyDeleteReference - https://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html
ReplyDeleteUpdated it sir.
Delete[5/15, 10:51 AM] : Because PCOS means increased oestrogen levels and osteoporosis is due to decrease in oestrogen levels.
ReplyDelete[5/15, 8:33 PM] Feedback from HOD OBG:
[5/15, 5:04 PM] KIMs Obg Prof Madhavi: Estrogen is osteo protective
[5/15, 5:04 PM] KIMs Obg Prof Madhavi: But osteoporosis can occur for any other reason
[5/15, 5:05 PM] KIMs Obg Prof Madhavi: So many are implicated in bone physiology
[5/15, 5:05 PM] KIMs Obg Prof Madhavi: Like parathormone, vit d, calcium
Okay sir. Thank you sir.
Delete[5/16, 12:53 PM] +91: Sir I added Behçet’s disease in my blog
ReplyDelete[5/16, 12:53 PM] +91 : Kindly see it.
[5/16, 8:39 PM] Rakesh Biswas: "Presented with the Complaints of :
1) Oral ulcers
2) Vaginal ulcers"
Since when?
[5/16, 8:40 PM] Rakesh Biswas: References need to be cited in text where you have borrowed quotes or paraphrased material from other online resources even if it's Wikipedia and not just cite Wikipedia in general in the reference
[5/16, 8:42 PM] Rakesh Biswas: "She got diagnosed with Behcets disease."
How? What criteria of Behchets does she satisfy? 🤔
[5/16, 8:44 PM] Rakesh Biswas: The rest of your recent additions were good but please cite proper reference in the text of your write up asap
[5/16, 10:23 PM] Rakesh Biswas: Still many areas in your write up that you have borrowed but not cited in text
ReplyDelete[5/16, 10:26 PM] Simran Dash 2015 Kims: I have written some in text sir instead of writing it in the end
[5/16, 10:27 PM] Simran Dash 2015 Kims: I thought maybe the renal failure made her more susceptible to infection
[5/16, 10:28 PM] Rakesh Biswas: Yes but there still many areas in your write up that are not your creation. Even if they are text book knowledge they need to be cited in text
[5/16, 10:29 PM] Rakesh Biswas: What renal infection did she actually have?
[5/16, 10:39 PM] Simran Dash 2015 Kims: It’s not mentioned in the actual blog sir about her exact infection. What I thought is since in females the incidence of renal infections is more and she already has renal failure because of the hemolysis that might have made her susceptible to the infection
ReplyDelete[5/16, 10:39 PM] Rakesh Biswas: Where is it mentioned that she has renal failure?
[5/16, 10:41 PM] Simran Dash 2015 Kims: It’s not mentioned sir. I think I just assumed it considering she has swelling and G6PD deficiency
ReplyDelete[5/16, 10:41 PM] Simran Dash 2015 Kims: Plus oliguria
[5/16, 10:45 PM] Simran Dash 2015 Kims: And she had Streptococcal infection at 14 years. Which makes her more probable for Post streptococcal Glomerulonephritis
[5/16, 10:53 PM] Rakesh Biswas: Yes but what proves that she had it? More definitive data to confirm that is not there in her given online record. So is there any point in assuming it?
[5/16, 10:53 PM] Simran Dash 2015 Kims: No sir
[5/16, 10:54 PM] Rakesh Biswas: Lesson here is always insist on the exact urinary volume before you take the data of oliguria as significant
[5/16, 10:58 PM] Simran Dash 2015 Kims: Sir what about her reactivation of EBV ? I couldn’t relate it to any of her complaints
ReplyDelete[5/16, 11:10 PM] Rakesh Biswas: Tell me more as to what has been mentioned around it in her original online record
[5/16, 11:15 PM] Simran Dash 2015 Kims: Sir what she has mentioned is that the rash in her face gets reactivated because of EBV?
[5/16, 11:15 PM] Simran Dash 2015 Kims: She gets it 2-4 times a year
[5/16, 11:16 PM] Simran Dash 2015 Kims: And cimetidine helped in the treatment of her rash
[5/16, 11:17 PM] Rakesh Biswas: How does she know she has EBV at that time?
[5/16, 11:17 PM] Rakesh Biswas: Placebo effect?
Inputs from Aditya Samitinjay PGY2:
ReplyDeleteThanks for the history Avinash and Simran.
The problem representation begins with characterising - who is the patient, what are her clinical problems and how long they have troubled her.
Epidemiologically, the patient is a 42F from Ohio who works as a freelance web designer and lives with her partner in her studio apartment. She has a keen interest in medicine
and frequently contributes to our learning. We do not know if she has any pets and nor do we know her recent travel history. Her menstrual and sexual history too would have helped to get
a better assessment of her quality of life.
Analysis of her first problem - "Migraine with Aura" - The sudden onset of unilateral throbbing pain are suggestive of Migraine. The triggers of her headache and associated nausea and
vomiting would have added weight to a diagnosis of migraine. The progression of her headache is unclear, did the intensity of a single paroxysm of headache progress or has it been
progressive over the past 8 years since her first "worst headache" of her life event.
To dissect Thuderclap headaches further (Source - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4416971/pdf/10.1177_2040622315579627.pdf)
SAH - Common things being common, no history of trauma makes SAH unlikely. For spontaneous SAH, a history of headache reaching maximium intensity within 1 hour and no neurological deficits
with LOC (according to Ottawa subarachnoid hemorrhage decision rule) would have favored a diagnosis of SAH. She never had LOC and her headaches remit with treatment and also were associated
with focal neurological deficits which makes SAH unlikey.
CVST (Cerebral Venous Sinus Thrombosis) - Would present with headache and fever (picket-fence pattern a possibility) and LOC with focal neurological deficits. Makes it unlikely. Here's more
on epidemiology of CVST - " A recently published study of 160 cases from the Canadian Pediatric Ischemic Stroke Registry calculated an annual incidence among children (up to 18 years) of 6.7
per million. Almost 50% of the sample were neonates (younger than 3 months), which indicates a higher incidence in that age group.6 Thus it appears that CVST is more common in the pediatric
and especially the neonatal age group.
CVST is a disease of young people. According to an Indian study, it is a major cause of stroke in young population with a mean age of 32.27 years and therefore should be considered in all
cases of young stroke and neurological syndromes in appropriate setting.5 In 1992, Ameri and Bousser reported a uniform age distribution in men with CVT, while 61% of women with CVT were
aged 20-35 years.7 This may be related to pregnancy or the use of oral contraceptives." (Source - https://jpma.org.pk/article-details/902?article_id=902)
ICH, Hypertensive Encephalopathy and Pituitary Apoplexy are also unlikely. All 3 would present with LOC and focal neurological deficits. Pituitary apoplexy is often seen during labour.
More inputs from Aditya Samitinjay PGY2:
ReplyDeleteChronic Migraine seems the most likely diagnosis. Here is some epidemiological data on the association of focal neurological deficits and speech abnormalities with chronic migraine -
"Only about 20% of migraine sufferers experience aura, usually (but not invariably) before the headache starts. Most aura is visual, consisting of a combination of positive visual phenomena (floaters,
flashes of light, moving or expanding zig-zag patterns, and so on) and negative phenomena (loss of vision causing blind spots). Many sufferers also experience sensory aura, consisting of tingling
and numbness, often spreading over the hand, arm, face, lips and tongue on one side of the body. Weakness, dysphasia, and other aura symptoms are rare.
(Source - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4416971/pdf/10.1177_2040622315579627.pdf)
Here's a case report of Acquired stuttering of speech in a patient with Acute Migraine attack - https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1046/j.1526-4610.2000.00025.x?sid=nlm%3Apubmed
Persistent worsening headaches - Raised ICP (tumour, abscess, CVST, idiopathic intracranial hypertension), Low ICP (post-puncture and spontaneous CSF leak) & Substance abuse/withdrawal.
Although incomplete, the history of her headaches is suggestive of a remitting pattern which is reponding to triptans. A chronic history of projectile vomiting, blurring vision and
progressively worsening headaches could suggest the diagnosis of Raised ICP. The CSF leak from her left nostril seems more like noise than signal to me. She apparently does not have a
history of substance abuse or withdrawal.
Brain Imaging would certainly help and I'm not sure why genetic studies were pursued instead of brain imaging. G6PD deficiency is an X-linked recessive trait and several hundred variants
exist which are harmless (Robbins & Cotran Textbook of Pathology 2015 & https://www.ncbi.nlm.nih.gov/books/NBK470315/). Only two variants are known to cause clinically apparent disease, G6PD- and G6PD Mediterranean. The former is
frequently associated with american black males and the latter in the Middle East. So epidemiologically the patient having clinically appareny G6PDD is extremely unlikely. Logically, it being
a XLR disease, both her parents must have had the culprit gene and a family history of hemolysis would certainly help.
More inputs from Aditya Samitinjay pgy2
ReplyDeleteRegarding MTHFR deficiency - "Methylenetetrahydrofolate Reductase (MTHFR) Deficiency is the most common genetic cause of elevated levels of homocysteine in the plasma (hyperhomocysteinemia)."
From the same article - Until recently, it was thought that MTHFR deficiency, by causing elevated homocysteine levels, led to an increased risk of venous thrombosis, coronary heart disease,
and recurrent pregnancy loss (8-11). However, more recent analysis has not found an association between elevated homocysteine levels and the risk of venous thrombosis or the risk of coronary
heart disease (12). MTHFR polymorphism genotyping should not be ordered as part of the clinical evaluation for thrombophilia, recurrent pregnancy loss, or for at-risk family members (4).
(Source - https://www.ncbi.nlm.nih.gov/books/NBK66131/)
Regarding AMPD1 deficiency - "AMP deaminase deficiency is one of the most common inherited muscle disorders in white populations, affecting 1 in 50 to 100 people.
Adenosine monophosphate (AMP) deaminase deficiency is a condition that can affect the muscles used for movement (skeletal muscles). In many affected individuals, AMP deaminase deficiency
does not cause any symptoms" (Source - https://ghr.nlm.nih.gov/condition/adenosine-monophosphate-deaminase-deficiency)
All in all this seems like Chronic Migraine to me. A history of the triggering factors would help, the duration of her headache and its aggravation with movements would strongly favor
a diagnosis of Migraine. TIA seems likely on an epidemiological basis - Her age is less than 60, she is a non diabetic and non hypertensive and she does not have a history of LOC.
The episodic feature of her headaches makes infections less likely, tumors too would have a persistent worsening headache. I wouldn't put my money on Metabolic disturbances or MELAS as all
3 genetic abnormalities are very common in normal population. All 3 have a recessive pattern of inheritance and in any case they don't explain her headaches.
Investigations required - Brain Imaging, which will most likely be normal. I wouldn't advise the other investigations the author has mentioned, just yet. The pretest probability of a CT/MRI
brain being normal (which I think would be high), enhances the post-test probability of migraine over all other conditions mentioned.