Heart failure - 1
CASE OF A 55 YEAR OLD FEMALE WITH HEART FAILURE
Submitted by : Simran Dash
MBBS- IV | Roll number : 153
I have been given this case data here :
Submitted by : Simran Dash
MBBS- IV | Roll number : 153
I have been given this case data here :
So according to the given data, the analysis made by me is as given below:
Age : 55 years
Sex - female
Occupation - agricultural labourer(works in paddy fields)
Chief complaints:
- Shortness of breath(since 3 months)
- Palpitations(since 2 months)
- Chest pain
- Swelling of legs upto ankle(since 1 week)
History in detail:
i) Shortness of breath:
- Onset - sudden
- Duration- 5 years and increased in intensity in the last 3 months
- Progression- gradually progressive (she is unable to carry out her daily chores apart from household activities thus making her Dyspnea grade -III according to NYHA classification.)
- Associated complaints -
- Orthopnea- since last 3 months, 1-2 episodes per week but in the last 10 days, every night 1 episode.
- Paroxysmal Nocturnal Dyspnea
- Wheezing
This indicates it could be a cardiac problem or respiratory problem.
ii) Palpitations:
- Character- Pounding which indicates -
- High output states such as anemia, beri-beri, thyrotoxicosis
- Structural abnormalities such as cardiomegaly, Left ventricular failure
iii) Chest pain:
- Onset - sudden
- Duration - 2 months
- Site - more on left side
- Radiation - non radiating
iv) Swelling of both the legs upto ankles(Bilateral pedal edema):
- Onset- sudden
- Duration-1 week
- Associated complaints- Oliguria (which relieved on medication)
This indicates it could be a cardiac problem or renal problem. But since there is no periorbital edema which is characteristic of Renal failure, we rule out primary renal cause. It could still be secondary to heart failure.
Past history: Had similar complaints 5 years back. She had a sudden onset of fever with cough which lasted for 5 days and got relieved on medication. It could have been Rheumatic fever. But there was no documentation of Rheumatic fever or the treatment taken for it.
From the history,
Factors in favour of Respiratory problem:
- Shortness of breath
- PND
- Orthopnea
- Wheeze
Factors not in favour of Respiratory problem are:
- No cough
- No hemoptysis
- No expectoration
So we rule out primary Respiratory involvement as of now. But it could be secondary to Right heart Failure (Cor- pulmonale).
Factors favoring Cardiac cause:
- Shortness of breath
- PND
- Orthopnea
- Palpitations
- Chest pain
- Pedal edema
- Oliguria
So on the basis of this I am of the opinion that the primary cause is in the Heart. Now it could be Left heart failure or Right heart failure. On the basis of symptoms,it is more suggestive of Left Heart Failure causing secondary Right heart failure.?
Examination findings:
- Respiratory system:
- Wheezing in right side (could be because of Heart Failure)
- Coarse crepitations in right side (indicating Pulmonary oedema)
These findings indicate that there could be Left Heart Failure.
2. CVS:
i) Peripheral Examination-
a) Pulse: Normal rate, Irregularly irregular rhythm with no apex pulse deficit, feeble.
This could be because of the following causes:
- Atrial Fibrillation(But there is no apex pulse deficit)
- Atrial Tachycardia
- Feeble pulse could be because of heart failure, shock, mitral stenosis
b) JVP: Increase in JVP with large 'a' waves. Causes for this are: Any condition in which more force is required for blood to enter into Right ventricle from Right atrium.
- Tricuspid stenosis
- Right Ventricular hypertrophy
- Right Atrial Tumour
- Pulmonary hypertension
ii) Examination of the precordium:
a) Inspection:
- Slight kyphosis of the back
b) Palpation:
- Apex beat is displaced downwards and outwards (indicating chronic Left Ventricular failure, could be because of the kyphosis also).
- Parasternal heave (indicates Right ventricular hypertrophy)
c) Auscultation:
- Loud S1 in mitral area (could be because of mitral stenosis).
- Splitting of S2 in pulmonary area with loud P2 (could be because of Pulmonary artery hypertension).
After examination, I am of the opinion that it could be a case of Left heart failure. The possible causes for it in this patient could be:
- Mitral stenosis
- Coronary Artery Disease
- Cardiomyopathy
- Anemia
- Left Atrial myxoma
Investigations done:
- CBP- showed Microcytic hypochromic anemia with neutrophilia (could be responsible for Chronic heart failure)
- RFT-
- Elevated blood urea
- Elevated uric acid
- Elevated Calcium
- Elevated Phosphorus
Patient also gives a history of oliguria.
This indicates that there is decreased blood supply to the kidneys causing them to shut down. This is because of Chronic heart failure.
- LFT-
- Elevated total bilrubin levels.
Heart Failure with reduced ejection fraction(HFrEF) causes two times increase in bilirubin levels than HFpEF.
- ECG-
- Absent p waves (Indicates atrial fibrillisation).
- Right axis deviation (indicates Right ventricular hypertrophy).
- ST elevation in V4,V5,aVR (indicating Lateral wall MI). Because of this, troponin levels were also investigated which was negative.
- Chest X ray (PA view)-
- Cardiomegaly
- Hypertrophy of left ventricle, right atrium and right ventricle.
- Mitralisation of heart means straightening of left border of heart and is due to-
i) Aortic Knuckle- Small
ii) Convexity due to dilated pulmonary artery (Pulmonary Hypertension)
iii) Left atrial appendage becomes prominent and produces a convexity.
4. Double contour of right border of heart
5. Evidence of pulmonary hypertension- Dilated pulmonary arteries
- 2D ECHO-
- Fish mouth appearance of the mitral valve (suggestive of Mitral stenosis).
- Calcified mitral valve
- Thickened immobile cusps
- Reduced valve area
After investigations I can confirm that this is a case of Left Heart Failure due to Mitral Stenosis.
Risk factors in this patient:
- Age- 55 years
- Sex- Female (greater risk for mitral stenosis)
- Had a previous similar history
Anatomical location of the root cause is in the mitral valve. The chordae tendinae and leaflets gets shortened to produce stenosis.
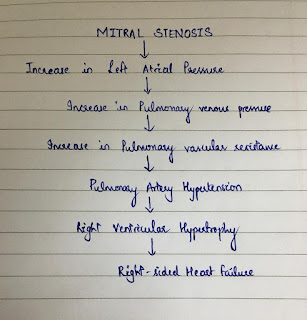
The most likely patholophysiology responsible for this patient is given as below:
Various etiologies responsible for Mitral Stenosis in this patient are:
- Rheumatic Fever (but there is no documentation)
- Ageing (causing calcification of the valve)
- Congenital mitral stenosis (secondary to parachute mitral valve or Lutembacher's syndrome).
Complications of Mitral stenosis in this patient are:
- Left Heart failure
- Pulmonary artery hypertension
- Atrial Fibrillation (but there is no apex pulse deficit)
- Renal failure (because of the LHF)
Addtional Investigations and Examinations required are:
- Doppler study - To record the pressure gradient across mitral valve and pulmonary artery systolic pressure.
- Cardiac catheterisation- To determine the hemodynamic status of the patient
- Characteristic murmur of Mitral Stenosis - mid diastolic rumbling murmur
- Opening snap might be present.
- Transoesophageal echocardiography
- TFT (Thyroid Function Tests) should be done.
- To diagnose rheumatic carditis, ASO titres are checked (which will be raised).
- Cardiac MRI - Gold standard to diagnose Heart Failure
- BNP levels (Brain Natriuretic Peptide): can help in the prognosis oh heart failure
Treatment modalities:
A) Pharmacological-
- Medical treatment (already received by the patient) Additional drugs required are
- Sacubitril/Valsartan (Entresto)
- Ivabradine
- Omecativ mecarbil (new cardiac myosin activator)
- Tolvaptan (oral vasopressin type 2 receptor antagonist) Advantage of this over loop diuretics is causes diuresis without any electrolyte imbalance.
2. Percutaneous mitral balloon valvuloplasty
3. Valvotomy or commissurotomy:
a) Open type (needs open heart surgery with cardio pulmonary by pass)
b) Closed type (more preferred)
4. Mitral valve reconstruction including annuloplasty
5. Valve replacement or prosthesis (Starr-Edwards ball valve or Bjork-Shelly disc valve)
6. Devices which can be used are:
- Cardiac resynchroniztion
- Implantable cardiac defibrillator
- Ventricular Assist Devices
B) Non pharmacological:
- Diet and nutrition mainly salt and fluid restriction.
- Adequate rest and Physical activity.
- Improve symptom recognition and self care behaviour
- Yoga, meditation may reduce the anxiety in patients and can also improve the breathing
- Continuous Positive Airway Pressure (CPAP) to improve daily functional activity and quality of life.
- Adequate disease managaement and follow up of the patient with Heart Failure can reduce readmission rates.
C) Prevention:
- Rheumatic Heart Disease:
- Primary- Penicillin prophylaxis can prevent an attack of rheumatic fever in a patient presenting with acute pharyngitis caused by Group A streptococcal infection.
- Secondary- To prevent further attacks by Group A beta hemolytic streptococcus in a patient who had a previous rheumatic fever.
References :
1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3331650/
2) https://www.ecrjournal.com/articles/non-pharmacological-management
3) Clinical methods of medicine by Arup Kumar Kundu
4) Hutchison’s clinical methods
5) Harrison’s principles of internal medicine
6) https://www.mayoclinic.org/diseases-conditions/mitral-valve-stenosis/symptoms-causes/syc-20353159
7) Davidson’s principles and practice of medicine
1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3331650/
2) https://www.ecrjournal.com/articles/non-pharmacological-management
3) Clinical methods of medicine by Arup Kumar Kundu
4) Hutchison’s clinical methods
5) Harrison’s principles of internal medicine
6) https://www.mayoclinic.org/diseases-conditions/mitral-valve-stenosis/symptoms-causes/syc-20353159
7) Davidson’s principles and practice of medicine
Auscultation findings
ReplyDeleteS1 and S2 heard
S3 is absent
okay. Thank you Bhavana. :)
Delete