Heart Failure-3
Case of a 30 year old male with Pulmonary Artery Hypertension
Submitted by- Simran Dash
MBBS- IV | Roll number- 153
I have been given this case data here to develop my understanding on the topic of heart failure.
My analysis for the above patient is as follows-
Age: 30 years
Sex: Male
Occupation: Shepherd (does not work now because of the dyspnea impairing his productivity.)
Chief complaints:
- Dyspnea since 15 days
- Bilateral pedal edema since 15 days
- Palpitations
- Dry cough since 2 months
Complaint in detail-
- Dyspnea:
- Onset- sudden
- Duration- 15 days (although he had similar episodes from October last year, intensity increased in the last 15 days)
- Progression- Gradually progressive
- Aggravating factors- Initially while working as a shepherd but later it has increased to breathlessness walking over a few short distances (NYHA grade 3 as of now)
- Relieving Factors- Rest
Causes of Dyspnea:

2)Bilateral pedal edema:
- Onset- sudden
- Duration- 15 days
- Site- Bilateral extending upto both knees
- Type- Pitting
- Associated with oliguria sine 2 days
The primary etiology could be in-
- Heart
- Kidneys
- Liver
There is also oliguria which could suggest a renal pathology. Or it could be secondary to Right heart Failure. There is also no periorbital edema so the primary pathology is probably not in the kidneys.
There are no findings in history to support cirrhosis of liver.
Could be Heart Failure.
- Onset- sudden
- Duration- Since October last year
- Character- Pounding
- Progression- persistent
- Aggravating factors- exertion
- Relieving factors- Rest
- Associated complaints-
- Dizziness with near blacking out episode (but never loss of consciousness)
- Profuse sweating
So the probable etiologies could be:
- Volume overload states because of the pounding nature. It could be-
- Anemia
- Wet beri-beri
- Thyrotoxicosis
- AV Fistula
2. Structural abnormalities of the heart:
- Congenital heart Diseases
- Cardiomegaly
- Left ventricular failure
- Aortic aneurysm
3. Miscellaneous:
- Postural Orthostatic Tachycardia syndrome (POTS)
- Brugada syndrome
These conditions are possible because of his near blacking out episodes and profuse sweating. This indicates stimulation of sympathetic nervous system particularly the vagus nerve.
4. Non cardiac etiology: Because of associated complaints like profuse sweating
- Stress
- Anxiety
This could also be because of stimulation of sympathetic nervous system. So there should be associated complaints to confirm anxiety like restlessness, irritability, insomnia,trembling of hands etc. Since there is no such complaints and he also says that his sleep remains undisturbed despite of having dyspnea we rule out anxiety as a cause.
4) Dry cough
- Onset- sudden
- Duration- 2 months
- Type- dry (without expectoration)
- Associated complaints-
- Wheezing at night (but sleep is undisturbed)
- No snoring
- There is no hemoptysis.
Causes of dry cough with nocturnal wheezing are:
- Asthma (no past history suggestive of Bronchial Asthma)
- Idiopathic pulmonary fibrosis (Also has SOB)
- Allergies
- Prolonged exposure to pollution,dust, chemicals (history is not suggestive of that)
So from history, I am of the opinion that it could be a case of heart failure. Most likely it is Right sided heart failure because he has no orthopnea and PND so Left heart failure is ruled out.
Past history-
- He has mental retardation.
On examination, the positive findings are:
- General examination: Has bilateral pitting type of pedal edema extending upto knees.
- Head and Neck examination:
- Sparse
- Less lustrous
- Premature graying
- Thinning of hair
This could be because of-
- Malnutrition
- Trichotilomania (because he is mentally retarded)
- Hormonal problems (Hypothyroidism)
- Vitamin B12 deficiency (can cause premature greying of hair)
- Metabolic disorders (can also cause premature graying)
- Oral examination:
- Poor periodontal status with severe calculus,
- Premature exfoliation of teeth
- Carious teeth, thick and pasty saliva
- White lesion on the right side of the tongue.
The above findings have been linked to oral candidiasis. Causes of which in this patient could be-
- Because of poor oral hygiene owing to his mental retardation state.
- Endocrine disturbances (Hypothyroidism)
- Vitamin deficiency
- Other findings:
- Very less facial hair
- No axillary hair
- Less pubic hair
- Cryptorchidism (undescended testes)
The above findings suggest Hypogonadism with Tanner stage 4 development which could be because of the following possibilities-
- Congenital Heart Disease (cryptorchidism)
- Hormonal problems
- Respiratory System:
- Wheezing is present.
- CVS examination:
- Pulse rate- 124 bpm (high) could be Tachycardia
- JVP- Raised with prominent 'a' wave. It could be due to
- Tricuspid stenosis
- Pulmonary Artery Hypertension
- Right Ventricular Hypertrophy
- Right atrial myxoma
ii) Examination of the precordium:
- Apex beat felt in the 5 th intercoastal space within mid clavicular line,well sustained,diffuse and confined to one intercoastal space.
- Visible pulsations over tricuspid and mitral areas.
- Right ventricular heave is present.
- S1 and s2 heard , loud p2.
- Holosystolic murmur of grade 3 intensity heard in pulmonary and tricuspid area.
The above findings suggest that the causes could be-
- Pulmonary artery hypertension because of the following causes-
- Loud P2
- Right ventricualar heave
2. Because of the holosystolic murmur it could be-
- Ventricular septal defect
- Mitral regurgitation
- Tricuspid regurgitation
3. COPD causing Cor pulmonale.
- CNS examination:
- The patient is conscious, coherent, cooperative and well oriented to time, place and person.
- He has a high stepping gait
- Pes cavus is also seen.
- Power is reduced in the proximal lower limb muscles.
- His deep tendon reflexes are very much reduced.
- He is little less attentive which could be due to-
a) Autism spectrum
b) Attention Deficit Hyperactivity Disorder
- Although his MMSE Score is 28 which indicates normal cognitive status.
The above findings suggest he could have-
- Friedrich's Ataxia (Findings suggestive are-
- Pes cavus (could also be because of Charcot- Marie- Tooth Disease - but no findings suggestive of that)
- Deep tendon reflexes are almost absent(very much reduced.) : Lower motor neuron lesion.
- Tachycardia
- Heart murmurs
- Weakness of lower limb muscles.
After examination, I came to the conclusion that he could have-
- Right heart failure due to Pulmonary Artery Hypertension (Group 1- Idiopathic)
- Friedrich's Ataxia
- Hypogonadism
- Oral candidiasis
Therefore, our data show higher estradiol, estradiol/testosterone ratio, lower testosterone, and progesterone were associated with increased risk of PAH. Meanwhile, higher estradiol was independently associated with higher mortality in men with PAH.
Causes for his problems could be-
- Storage diseases
Glycogen storage disease-1 (GSD-1) Can cause Pulmonary artery hypertension, Hypogonadism
PAH is a rare but highly fatal disease that has been associated with GSDI. Given the rarity of both GSDI and PAH, the exact incidence of PAH in patients with GSDI is difficult to quantify
Hypogonadotropic hypogonadism is an important complication in glycogen storage disease (GSD) type 1 and incorporating clinical and/or biochemical screening of the hypothalamic–pituitary–gonadal axis may be important in the management of this disease.
- Mitochondrial diseases
- Genetic disorders
Investiagtions:
- CBP:

Normocytic normochromic anemia(could be responsible for his palpitations)
- Thyroid Function Tests

- Chest X ray

Shows cardiomegaly, Dilated Pulmonary artery
- LFT:

Elevated Alkaline phosphate levels
- Blood sugar

Elevated fasting blood sugar and high HbA1c levels (complication of Fredrich's Ataxia is Diabetes)
- ECG:

There is sinus tachycardia, irregular rhythm, inverted T waves in leads V1-V5.
- Colour Doppler:

Dilated Right atrium and Right ventricle (could be responsible for cardiomegaly)
After investigations I can confirm that this is a case of Right Heart Failure with Idiopathic Pulmonary Artery Hypertension. To confirm my other possible diagnoses in this case, additional investigations required are:
- Coronary angiography
- Cardiac MRI - To confirm the PAH
- CNS examination-
- IQ Testing
- Nerve conduction study
- Examination of dorsal tracts
- Hormonal assay- To determine whether it is primary or secondary testicular failure.
- FSH levels
- LH levels
- Testosterone levels
- GnRH levels
In a person with primary hypogonadism, the levels of testosterone will be less.
Whereas in secondary hypogonadism,

- Whole genome sequencing to find out any mutations like FXN gene on chromosome 9 for Friedrich's ataxia.
- Culture to confirm oral candidiasis
- Nerve conduction study and EMG to confirm Friedreich ataxia.
Management:
A) Pharmacological modalities: The following are already taken by the patient-
- Tab pan 40 mg po od
- Inj lasix 20 mg iv bd
- Inj thiamine 1 amp in 100 ml ns
- Inj optineuron 1 amp in 100 ml ns
- Tab sildenafil 10 mg po bd
- Tab benfomet plus od
Additional treatment modalities required are
i) Medical-
- Topical Nystatin or miconazole for Oral Candidiasis.
- Vasodilators like epoprostenol (Flolan, Veletri)
- Guanylate cyclase stimulators like Riociguat. It relaxes the pulmonary arteries and lowers pressure within them.
- Digoxin
- Endothelin receptor antagonists like Bosentan, Ambrisentan.
ii) Surgical-
- Atrial Septostomy- In this procedure, a window is created between the upper left and right chambers of the heart to relieve the pressure on the right side of the heart.
- Transplantation- A lung or heart-lung transplant can be done especially for younger people who have Idiopathic Pulmonary Artery Hypertension.
B) Non Pharmacological modalities:
- Plenty of rest.
- Stay as active as possible.
- Eat healthy according to Harvard plate
- Vaccines for Inflenza, pneumonia should be taken.
- Orthotics with extra depth shoes for pes cavus.
- Brushing twice daily for oral candidiasis.
Complicatons of Pulmonary Artery Hypertension in this case:
- Right Heart Failure
Anatomical location of the root cause is in the pulmonary artery.
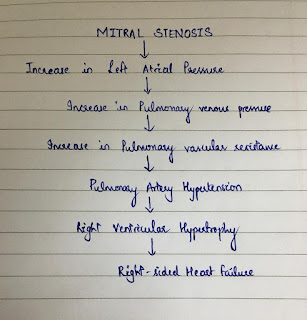
Pathophysiology which could explain this is :

Aetiology for this case is already discussed above.
Things which I did not understand in this case are:
- How was he diagnosed of having oral Candidiasis? Is there a picture which could give us more insight on his oral lesions.
- If he had this problem since last year October, why did he not approach any doctor?
References:
- Harrison's principles of internal medicine
- Davidson's principles and practice of medicine
Hello Simran,
ReplyDeleteA very thorough and terrific analysis of the case. Well presented and I'm glad you also went through Dr. Vidya's blog to get both versions of the history taken.
I have previously commented on a few other students' blogs who analysed the same case and all of your work has been impressive.
I'd like to start off with understanding the importance of epidemiology of the patient in providing better analysis, differentials and improved patient care. This is a 30M who worked as a shepherd, was able to function well and asymptomatic until last October when he noticed he became breathless when walking uphill. The patient remembered this because it is unusual to his daily keeping. The fact that he also reported palpitations with these episodes of exertional dyspnoea highly favor a cardiac cause for his symptoms. The fact that they were pounding, exertional and relieved with rest suggest a volume overload condition and you can simply organise them by LVOTO (left ventricular outflow tract obstruction) such as AS and HOCM. RVOTO such as Pulmonary Embolism, PS and PAH. Or restrictive cardiac conditions such as Constrictive Pericarditis. It also is important to analyse the tempo of the disease. This is a chronic condition and so conditions like Pulmonary embolism and Constrictive pericarditis or Pericardial Effusions are unlikely. Allied to this, add the data that his palpitations are persistent and chronic and this can push arrhythmias down the list. Volume overload conditions take precedence now. Now ally this with his blacking out and you can prioritise LVOTO or RVOTO over all other hyperdynamic or volume overload states because OTO conditions decrease stroke volume (particularly on exertion) and also can reduce coronary filling which can cause blacking out.
To recap, with the above analysis, we can safely rule out anemia, thyrotoxicosis ans wet beri beri because they are extremely unlikely to cause syncope.
I'm also skeptic about considering a renal cause because the history is suggestive of a progressive, exertional condition with highly specific cardiac symptoms. A liver failure too would be unlikely, going by the same analogy.
I also do not think he has mental retardation. The man finished school upto class 7 and is able to handle his own finances. You've quite frequently mentioned mental retardation, which may alter your thinking.
Do you see the approach I've taken here ? Im no expert and I'm just as enthusiastic to learn as you are but I believe the summarising the patient's history by creating a problem representation would advance your analysis leaps and bounds. This first involves understanding the epidemiology of the patient, followed by the tempo of the disease and the clinical syndrome.
With all these in mind, several conditions you've listed can be easily ruled out and you'd be left with only a handful of diagnoses which should narrow down further after performing the physical examination.
It's also important to consider the odds of a test being positive or negative in a particular patient. The pretest probability of this man having abnormal thyroid, liver and renal function tests are very low.
It's a great start you made. I'm impressed and thank you for reaching me about PAH drugs and where they act. Great work overall.