Case discussion on mitral stenosis
Active learning points from the discussion on the following case:
Details of the patient are given below:
Details of the patient are given below:
My analysis for the above patient is given in the link below:
https://rhea9895.blogspot.com/2020/05/heart-failure-1.html?m=1
https://rhea9895.blogspot.com/2020/05/heart-failure-1.html?m=1
29/05/20, 10:07:00 PM] Student3:
Question:
How does elevated total bilirubin as in this case affect the outcome of cardiovascular diseases like heart failure?
[29/05/20, 10:10:17 PM] Student4: Heart failure might have caused liver dysfunction leading to raised bilirubin levels
[29/05/20, 10:16:23 PM] Student3: What is the effect of higher bilirubin levels on the risk of causing heart failure in those people?
[29/05/20, 10:23:53 PM] Student3: The question is effect of elevated total bilirubin on risk of heart failure...not vice versa
[29/05/20, 10:27:10 PM] Student4: This study shows there is inverse relationship between them
https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/1471-2261-12-16
https://bmccardiovascdisord.biomedcentral.com/articles/10.1186/1471-2261-12-16
[29/05/20, 10:28:14 PM] Student3: Yes
[29/05/20, 10:28:53 PM] Student3: Even this source says it-it-https://www.google.com/amp/s/www.medicalnewstoday.com/amp/articles/321874
[29/05/20, 10:30:31 PM] Student4: But in this case he has elevated bilirubin how does that explain his heart failure
[29/05/20, 10:30:37 PM] Student3: Yes
[29/05/20, 10:30:41 PM] Student3: But why?
[29/05/20, 10:33:07 PM] Student5: Okay, the thing is what u said was right but heart failure itself might cause increased levels of bilirubin
[29/05/20, 10:33:29 PM] Student4: Yes
[29/05/20, 10:33:32 PM] Student3: Yes...it can👍
[29/05/20, 10:33:44 PM] Student5: Heart failure can rob your liver of the blood it needs to work. The fluid buildup that comes with it puts extra pressure on the portal vein, which brings blood to your liver. This can scar the organ to the point where it doesn't work as well as it should.
[29/05/20, 10:34:37 PM] Student3: Maybe this is the reason for elevated bilirubin in this case then...
[29/05/20, 10:35:05 PM] Student5: Maybe
[29/05/20, 11:05:59 PM] Student6: Yes.. heart failure can cause liver failure which causes raised bilirubin... But is the patient having the heart failure of the severity that is required to cause liver failure to cause increased bilirubin levels...?
[30/05/20, 9:58:33 AM] Post Residency PG1: Good question.
So what are the indicators to severe heart failure in this patient? Does she have right ventricular failure alone or also has left ventricular failure? Does left ventricular failure happen in pure mitral stenosis?
[30/05/20, 5:03:32 PM] Post Residency PG1: Please share scientific links to any statement you make. Particularly the comment "overload on left ventricle"
[30/05/20, 5:05:48 PM] Student12: https://www.mdmag.com/journals/cardiology-review-online/2007/may2007/may-2007-mallis-commentary
[30/05/20, 5:06:03 PM] Post Residency PG1: This sounds better
[30/05/20, 5:06:35 PM] Post Residency PG1: Please quote from the relevant portions that you want us to focus on
[30/05/20, 10:31:37 AM] Student6: Hepatojugular reflex is an indicator of severe heart failure. Disorientation , fatigue and fluid retention may be the the symptom we need to see if the disease is severe.
[30/05/20, 11:07:28 AM] Student8: Positive Hepatojugular reflex is an indicator of complete heart failure or right heart failure?
[30/05/20, 11:11:44 AM] Student9: it could be a marker of both elevated left-sided and right-sided filling pressures.
Hence, hepatojugular reflux should not be considered diagnostic of any particular condition, but an indication that the right ventricle cannot accommodate an increased venous return
[30/05/20, 11:12:02 AM] Student9: Constrictive pericarditis, right ventricular failure (commonly due to infarction), and restrictive cardiomyopathy are conditions that frequently produce a positive hepatojugular reflux
[30/05/20, 11:12:46 AM] Student6: It is an indication of heart failure of all the etiologies. It is not specific..to one..
[30/05/20, 11:12:55 AM] Student9: *Left ventricular failure also produces this sign, but usually when the PCWP is more than 15 mmHg.
***Cardiac tamponade does not lead to a positive hepatojugular reflux.
[30/05/20, 11:17:14 AM] Student8: Okay
[29/05/20, 11:08:13 PM] Student1: His apex beat is displaced that means he has a chronic heart failure
[29/05/20, 11:10:09 PM] Student4: Then he should have severe MS
[29/05/20, 11:10:59 PM] Student1: We don’t know the surface area of Mitral valve right?
[30/05/20, 9:55:01 AM] Post Residency PG1: What does apex displacement have to do with severity of Mitral Stenosis?
[30/05/20, 9:58:39 AM] Student4: No sir I meant is it severe MS leading to chronic heart failure which affected the liver also
[30/05/20, 10:00:15 AM] Post Residency PG1: Severe pure MS causes which sided heart failure?
[30/05/20, 10:00:53 AM] Student4: Initially left sided failure and later even right heart failure
[30/05/20, 10:03:36 AM] Student7: I think it's initially right sided failure
[30/05/20, 10:03:51 AM] Student4: How?
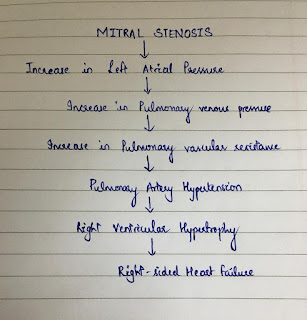
[30/05/20, 10:05:09 AM] Student4: Mitral stenosis leads increase in left atrial pressure which leads in increase in pressure in pulmonary veins and a artery and right ventricle
Leading to right ventricular failure
[30/05/20, 10:05:32 AM] Student7: Initially left atrial pressure is increased to maintain thecardiac output which increases pulmaru capillary wedge pressure and resulting pulmonary HTN leads to right heart failure
[30/05/20, 10:05:52 AM] Student7: Yes
[30/05/20, 10:07:51 AM] Student4: In this case initially he had features of left heart failure then eventually he developed pedal Edema
[30/05/20, 10:08:20 AM] Post Residency PG1: Elaborate
[30/05/20, 10:10:41 AM] Student4: In this case of mitral stenosis pt initially presented with Dyspnea which Is symptom of lt heart failure then later he developed pedal edema (feature of rt heart failure)
If mitral stenosis is due to rt heat failure initially then the pt should present with pedal edema first???
[30/05/20, 10:11:58 AM] Post Residency PG1: Dyspnoea is a symptom of failure of which part of the left heart?
[30/05/20, 10:12:42 AM] Post Residency PG1: Left ventricle or left atrium? Particularly in mitral stenosis?
[30/05/20, 10:12:53 AM] Student4: Left atrium
[30/05/20, 10:16:37 AM] Post Residency PG1: Yes in pure mitral stenosis there is no left ventricular failure. Only left atrial failure due to left atrial outflow obstruction.
How does it lead to different grades of dyspnoea?
[30/05/20, 11:55:42 AM] Student11: Sir In the case of severe mitral stenosis, there is increase in the pulmonary venous pressure which transmits as a back pressure to the pulmonary arteries
which leads to edema. This is the cause for Dyspnoea
[30/05/20, 5:19:01 PM] Student13: Elevation of left atrial pressures leads to pulmonary venous hypertension, which leads to reduced compliance of the lungs and a decrease in vital capacity, resulting in Dyspnea.
Dyspnea on exertion may be related to an inability to increase the cardiac output due to impaired left ventricular filling leading to a low end diastolic volume.
[30/05/20, 5:21:01 PM] Post Residency PG1: Yes but what is the mechanism of that feeling of dyspnoea which is defined as an abnormal awareness of one's own normal breathing
[30/05/20, 6:08:42 PM] Student13: "It is thought that three main components contribute to dyspnea: afferent signals, efferent signals, and central information processing. It is believed the central processing in the brain compares the afferent and efferent signals; and dyspnea results when a "mismatch" occurs between the two: such as when the need for ventilation (afferent signaling) is not being met by physical breathing (efferent signaling)."
Reference:
Harrison's Principles of Internal Medicine (Kasper DL, Fauci AS, Longo DL, et al. (eds)) (16th ed.). New York: McGraw-Hill.
[30/05/20, 6:10:03 PM] Student13: Does Pulmonary venous hypertension lead to Pulmonary interstitial edema?
[30/05/20, 6:12:04 PM] Student13: If yes,
The development of interstitial edema could lead to the stimulation of C-fibers.
C-fibers are unmyelinated afferent nerve fibers that originate in J-receptors located in small airways and near alveolar capillaries; they are stimulated by mechanical and chemical factors. The stimulation of the J-receptors causes a reflex increase in breathing rate, and is also thought to be involved in the sensation of dyspnea.
[30/05/20, 8:16:53 PM] Post Residency PG1: So would the J receptors and C fibers be stimulated also by airway resistance as that also causes dyspnoea? Let's look at scientific studies and not just text book assumptions.
[30/05/20, 10:59:14 PM] Student13: Effects of bronchoconstriction and external resistive loading on the sensation of dyspnea:
This study compared the sensation of difficulty in breathing during isocapnic voluntary hyperventilation in six normal subjects.
"To clarify the role of vagal afferents on the genesis of dyspnea during both forms of obstruction to airflow, the effect of airway anesthesia by lidocaine aerosol inhalation was also examined after histamine and during external resistive loading."
"Histamine inhalation significantly increased the intensity of the dyspneic sensation over the equivalent external resistive load at the same levels of ventilation and occlusion pressure during voluntary hyperpnea. Inhaled lidocaine decreased the sensation of dyspnea during bronchoconstriction with no change in Raw, but it did not significantly change the sensation during external resistive loading. These results suggest that afferent vagal activity plays a role in the genesis of dyspnea during bronchoconstriction."
[30/05/20, 11:01:27 PM] Post Residency PG1: And where do the vagal afferents relay to convey this sensation of dyspnoea? Also are they connected to the J receptors in the alveoli or some other receptors?
[30/05/20, 11:09:55 PM] Student13: Afferent information from reflex stimulation of the peripheral sensors (chemoreceptors and/or vagal C fibers) is processed/relayed centrally in the limbic system, especially the insular area and sensorimotor cortex.
A perturbation in the ventilatory response due to weakness, paralysis, or increased mechanical load generates afferent information from vagal receptors in the lungs (and possibly mechanoreceptors in the respiratory muscles) to the sensorimotor cortex and results in the sensation of dyspnea.
[30/05/20, 11:10:59 PM] Student13: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2972628/
[29/05/20, 11:12:52 PM] Student2: Don't we need to know where the apex is displaced? Outward only or downward and outward? That'll tell us which ventricle is effected
[30/05/20, 9:53:13 AM] Post Residency PG1: Which ventricle?
[29/05/20, 11:13:15 PM] Student4: Down and out
[29/05/20, 11:13:32 PM] Student1: It’s displaced outward and downward and is in the anterior axillary line
[29/05/20, 11:13:39 PM] Student4: Seen in 6 Th intercostal space in ant axillary line
[29/05/20, 11:13:46 PM] Student3: Its downward n outwards as given in the case report
[29/05/20, 11:13:59 PM] Student3: Yes
[29/05/20, 11:13:35 PM] Student2: So left ventricle hypertrophy
[29/05/20, 11:13:59 PM] Student1: Yeah.
[30/05/20, 9:52:45 AM] Post Residency PG1: Or left ventricular dilatation?
[30/05/20, 10:19:50 AM] Student2: Yes sir. We should consider that as well
[30/05/20, 10:20:49 AM] Post Residency PG1: That would mean she has left ventricular failure and not pure mitral stenosis?
[30/05/20, 10:28:35 AM] Student2: If we consider the displacement of the apex, then yes sir.
[30/05/20, 9:55:42 AM] Post Residency PG1: Chronic left ventricular failure gives rise to left ventricular dilatation? Why?
[30/05/20, 10:26:20 AM] Student7: Sir what is the reason for cardiomegaly in this case?
[30/05/20, 11:50:49 AM] Student10: Isn't it because of ventricular remodeling??
Comments
Post a Comment