32 years old male with c/o yellowish discolouration of eyes since 1 and 1/2 months
- Yellowish discolouration of eyes since 1 and 1/2 months.
- SOB since 10 days.
- Cough since 5 days.
- Fever since 2 days.
History of present illness- The patient was apparently asymptomatic 6 months ago. Then he developed yellowish discolouration of eyes (with a TB- 6 mg/dl). Following which he got scared and stopped consuming alcohol for 3 months. Then his bilirubin levels came down following which he resumed consuming alcohol.
He drank alcohol and fought with his friend and injured his right arm sustaining a fracture to his right arm which was left untreated. His yellowish discolouration of eyes recurred in 1 month hence he stopped consuming alcohol.
H/O GTCS 1 month ago after stopping alcohol for about 10 days- ? Alcohol withdrawal. Patient assumed that his seizures would stop if he resumes consuming alcohol thereby started drinking again.
1 month ago, his yellowish discolouration of eyes increased so he stopped again. But the discolouration progressed and his entire body turned yellow in 1 month.
15 days ago, Patient’s attenders burnt his right arm in superstitious belief that his jaundice would come out through the burnt area.
C/O pedal Edema, abdominal distension since 6 days.
C/O productive cough since 5 days
C/O SOB (intermittent) since 5 days.
C/O fever since 2 days- which was low grade.
No h/o cold.
No h/o decreased urine output.
Past h/o: No h/o DM, HTN, TB, BA, Epilepsy, CVA, CAD.
Family h/o: No similar complaints in family
No h/o DM, HTN, TB, BA, Epilepsy, CVA, CAD.
Personal h/o:
Diet- mixed
Appetite- Normal
Sleep- Adequate
Bowel and Bladder movements- Regular
Regularly consumes 90-180 ml of alcohol since the last 15 years.
Occasionally chews tobacco.
General examination:
He is conscious, coherent, cooperative, moderately built and moderately nourished.
Pallor- Present

Icterus- Present

Cyanosis- Absent
Clubbing- Absent
Lymphadenopathy- Absent
Pedal Edema- Present upto legs

Vitals:
Temperature- 99 F
PR- 110 bpm
BP- 140/90 mm Hg
RR- 20 cpm
SpO2- 100% @ RA
GRBS- 176 mg/dl
Systemic Examination:
P/A: Soft, Non tender, No palpable organomegaly
Bowel sounds heard.
Flapping tremors present.

CVS- S1,S2 sounds present. No murmurs
RS- BAE+, NVBS heard
CNS- NAD
Provisional Diagnosis:
? ACUTE ON CHRONIC LIVER DISEASE
HEPATIC ENCEPHALOPATHY- GRADE I
HYPOKALEMIA
Investigations:
Serology- Negative
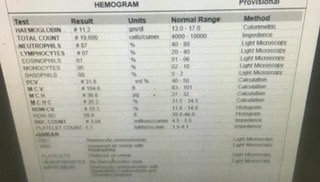
Hemogram-
LFT-

RFT-
RBS-

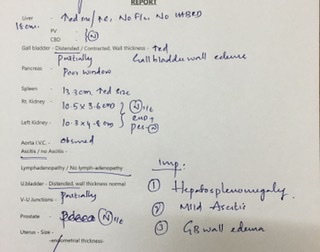
USG Abdomen-
CXR- PA view

ECG-

ABG-

TREATMENT:
1. INJ. LASIX 40 mg I.V./BD
2. TAB. ALDACTONE 25 mg PO/BD
3. SYP. LACTULOSE 10 ml P/O H/S
4. Temperature charting 4th hourly
5. Tepid sponging SOS
6. INJ. VIT. K 10 mg slow I.V./OD
7. SYP. ASCORYL-LS 10 ml PO/BD
8. SYP. POTCHLOR 10 ml in 1 glass of water PO/BD
Comments
Post a Comment