42 years old female with complaints of SOB since 3 months
- SOB since 3 months
- Cough since 10 days
- Fever since 7 days
- Decreased urine output since 2 days.
History of present illness: The patient was apparently asymptomatic 3 months ago. Then she developed SOB which was insidious in onset, progressive in nature, associated with wheeze and orthopnea. SOB was of Grade II-III.
Then she developed cough 10 days ago which was associated with exacerbation - mucoid, minimal, non blood stained, non foul smelling. Aggravated on lying down and relieved on sitting position.
Then she developed fever 7 days ago- insidious in onset, high grade, non progressive, relieved with medication.
She developed decreased urine output in the last 2 days.
- No c/o chest pain.
- No h/o myalgias.
- No h/o loss of taste or smell sensation.
- No c/o burning micturition, loose stools, vomitings.
Past h/o: H/O TB 10 years back. She took ATT for 6 months.
H/o similar complaints for the last 6 months. She is on inhalation since 10 days SOS.
H/o exposure to biogas since the last 25 years.
Not a k/c/o DM, HTN, Asthma, Epilepsy, CAD, CVA.
Family h/o- Not significant
Personal h/o-
Diet- Mixed
Sleep- Adequate
Appetite- Normal
Bowel and Bladder habits- Oliguria since last 2 days.
Normal bowel habits.
No addictions.
General Examination: She is conscious, coherent, cooperative well oriented to time, place and person. She is moderately built and moderately nourished.
Pallor- present
No icterus, cyanosis, clubbing, lymphadenopathy, Edema.
Vitals:
Temperature- 99.5 F
PR- 120 bpm
BP- 140/90 mm Hg
RR- 39 cpm
SpO2- 99% @ RA
GRBS- 141 mg/dl
Systemic Examination:
RS- BAE+, NVBS heard
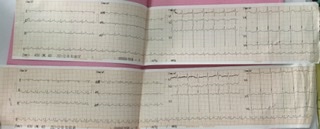
CVS- S1, S2 sounds heard. No murmurs.
GIT- Soft, non tender, Bowel sounds heard.
CNS- NAD
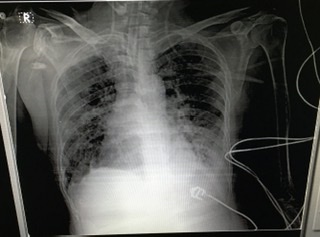
Provisional Diagnosis- ACUTE EXACERBATION OF COPD SECONDARY TO ?CAP
WITH TYPE -II RESPIRATORY FAILURE
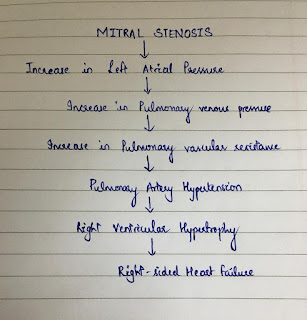
WITH SEVERE PAH-II
WITH POST TB SEQUALAE
WITH DENOVO HTN
WITH ?TIA
WITH MODS (DIC)
Investigations:
1) Summary of all investigations done from 15/12/21 to 18/12/21
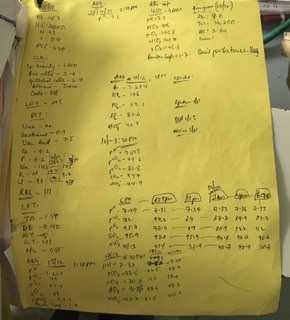








Comments
Post a Comment